cast away

I awoke to pitch black darkness.
The voices were close. And interspersed with laughter.
My cerebral cortex quickly determined the voices were causing each other to laugh; and coming from two lone individuals.
They seemed friendly.
But I wanted to scream at them for awakening me from the depths of my restless slumber; yet I hadn’t quite determined if they were real.
I wasn’t even certain where I was.

As I stared into the darkness surrounding me, my eyes began to accommodate as the voices continued in their laughter.
My body felt heavy. My mind was confused.
Instinctively, I bolted straight up from my position; I realized I was lying in bed. Unaccustomed to its small size, I nearly tumbled to the ground.
In the midst of the darkness, my neurons began flashing in an electrical brilliance, trying to understand where in person, place, and time I was.
My right arm reached across my body as the fog in my mind abruptly lifted.
The restless slumber I had been inhabiting came to a crashing halt, as my thumb flicked the push-button on my phone to reveal “2:07PM”.
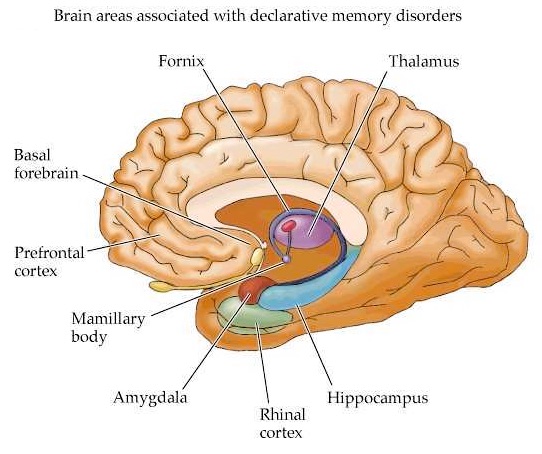
In that moment, my hippocampus determined I was located in the 2nd floor call room of the hospital.
A cataclysmic series of events brought me to be located in person, place, and time in the 2nd floor call room of the hospital on that July afternoon at 2:07PM.
Twelve nights had passed since I was shipwrecked on Night Float alone.

The plan, as it had been outlined to me several weeks earlier, would revolve around me undertaking a never-before-attempted solo excursion on Night Float.
My immediate fears had been squelched by promises of rearranged schedules and responsibilities, a junior resident as an occasional wingman, and deeply bound faith by my superiors that I was the only physician who could succeed in this plan.
My Ego led me to believe I could handle it.
But on Night Float, or “Black Betty” as I like to call her, all plans go quickly to hell.

Between the hours of 7PM and 7AM, a major metropolitan hospital is unlikely to have significant periods of down time. Instead, it becomes the breeding ground for Chaos Incarnate.
Which is directly where I found myself for the first 2 and ½ weeks of my third year of Residency.
Alone with Black Betty.
Nestled in her bosom.
cast away.
And longing for rescue.

By the beginning of my second week of Night Float as a PGY-3, my confidence had been rattled, but not deteriorated, like a rock face in the ocean having succumbed to centuries of waves bearing down it.
PGY-2 had been tortuous, but while working so many random weekend days and nights had crippled my life outside of the hospital, they had shaped my abilities as a physician, both in and outside of the hospital.
Ultimately, nothing could have prepared me to be cast away.

Another senior resident had been assigned to work on Night Float with me originally, but that had fallen through due to her unforeseen circumstances.
Then a thorough review of the remaining options turned up the following: unleash Magneto into the depths of Chaos Incarnate alone and see what happens.
{Note: I was assigned a junior resident as a “life vest” for a few of the nights, but he had to leave by midnight, like a mirage, to leave me alone, carrying 4 pagers, anxiously awaiting the next sunrise.}
At times over those 2 and ½ weeks, Magneto conquered the tasks set before him. But many a times, Black Betty rattled him to his core.
The toll of spiritual, emotional, professional, personal, and existential fatigue came to a head on the day I awoke at 2:07PM in the hospital call room
I found myself there not because I longed for the sweet caress of a crisply dry-cleaned set of linens, but because I had left my apartment the previous night in a fugue state.
Said fugue state resulted in me dropping my keys through the hole in the bottom of my book bag; they came to a clattered resting place in my building’s entryway.
I was none the wiser because NIN’s “Terrible Lie” was blaring through my ear buds.
Only when I rummaged through my book bag for an hour the following morning, proceeded to walk to my apartment hoping to find the keys lying on the sidewalk like a trail of bread crumbs, and had left two babbling and pleading voice messages on my landlord’s answering machine, did I begrudgingly saunter back to the hospital.

So when I awoke to the jovial laughter of two newly reunited long-lost colleagues, I hoped to find a message on my phone indicating the safe recovery of my highly-sought after keys.
Alas, at 2:07PM, there were no messages on my phone.
Nor were there any messages at 6:30PM when the melodic alarm emanating from my iPhone jostled me awake again. My mind was still cloudy. My body was still aching.
But Black Betty wanted another go.

So I meandered from the call room into the locker room, proceeded to strip down from my wrinkled scrubs and hit the showers.
The searing ice cold water streaming from the shower head caused my body to shiver, reminding me of my morning showers in Dominica, but I managed to cleanse the fine film of solitude from each and every square inch of my being.
I dried off, turned my socks and boxer-briefs inside out, and slowly pulled on a new set of pressed green scrubs.
As I passed the half-length mirror in the locker room, I quickly assessed my physical form and found my two-week-old beard to be quite fitting a man so unfamiliar with his surroundings.

I wondered if I would ever be found…